CMS Proposes Changes to Physician Self-Referral Regulations to Promote Value-Based Health Care
CMS Proposes Changes to Physician Self-Referral Regulations to Promote Value-Based Health Care

CMS Proposes Changes to Physician Self-Referral Regulations to Promote Value-Based Health Care
Key Points:
- The Centers for Medicare and Medicaid Services (CMS) have issued a long-awaited proposal to reform the Physician Self-Referral Law’s (Stark Law’s) regulatory exceptions and to provide updated guidance for physicians and health care providers and suppliers whose financial relationships are subject to the Stark Law.
- The goals of these reforms are to modernize and clarify the Stark Law regulations in order to (a) alleviate the undue impact of the Stark Law on parties that participate in alternative payment models and other novel financial arrangements, (b) better facilitate patient care coordination and management among providers and other health care delivery partners, and (c) advance the transition from a payment model that compensates on a fee-for-service basis to one that rewards quality outcomes and value achieved.
- Simultaneously, the U.S. Department of Health and Human Services Office of Inspector General (OIG) released its own highly anticipated proposed reforms to the Anti-Kickback Statute safe harbors, also with the goal of advancing value-based care. Akin Gump’s Client Alert on the Anti-Kickback Statute proposals is available here.
- Comments to CMS’s proposal are due Dec. 31, 2019.
Discussion:
On October 9, 2019, CMS issued a proposed rule to update the Stark Law’s regulatory exceptions.1 With this proposed rule, CMS aims to update the Stark Law regulations to better reflect the realities and trends of modern health care. The following are some of the most significant proposals:
- First, CMS proposes to update the Stark Law regulations to create new exceptions for “value-based arrangements” (as defined below) in order to better facilitate innovation and enable the transformation of the health care system towards value-based care—and away from a fee-for-service model of payment.
- Second, CMS is seeking comments on the role of price transparency in the context of the Stark Law and whether to require cost-of-care information at the point of referral for an item or service.
- Third, CMS hopes to continue to facilitate the adoption of electronic health record (EHR) technology and decrease cybersecurity risk in the health care industry by providing greater flexibility to existing Stark Law exceptions and through the creation of a new exception for the donations of certain cybersecurity technology.
- Fourth, CMS proposes to clarify terminology and concepts critical to the Stark Law in order to ease some of the considerable burden of compliance with the self-referral law and regulations.
CMS proposed changes to make it clear that the agency, while focused on preventing abuse, is emphasizing innovation in health care and seeking to identify and address any undue impacts and burdens of compliance with the Stark Law. In addition, with the proposed regulation, CMS aims to promote coordination and alignment with the OIG’s concurrently released proposed Anti-Kickback safe harbor rule in order to ease the compliance burden in the industry.
New Exceptions for Value-Based Arrangements
To facilitate the new value-based exceptions, CMS proposes new defined terms (42 CFR § 411.351).
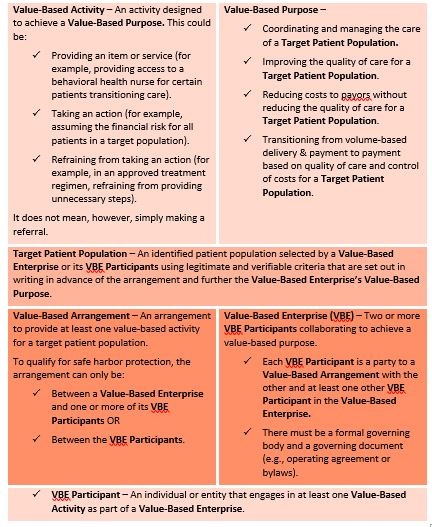{kind=link}
In the rulemaking, CMS proposed to create three new exceptions for value-based arrangements. These exceptions apply “regardless of whether the arrangement relates to care furnished to Medicare beneficiaries, non-Medicare patients, or a combination of both.”2
1. Full Financial Risk Exception (Proposed 42 CFR § 411.357(aa)(1)): This exception protects remuneration paid under a value-based arrangement between VBE participants in a value-based enterprise that has assumed “full financial risk” for the cost of all patient care items and services covered by the applicable payor for each patient in the target population for a specified period of time. To satisfy this exception, VBE participants must meet the following requirements:
- The value-based enterprise is financially responsible (or is contractually obligated to be financially responsible within the first six months of the arrangement) for the cost of all patient care items and services (e.g., via capitation payments or global budget payments).
- The financial risk must be prospective.
- The remuneration is for or results from value-based activities undertaken by the recipient of the remuneration for patients in the target patient population.
- The remuneration is not an inducement to reduce or limit medically necessary items or services.
- The remuneration is not conditioned on referrals of patients who are not part of the target patient population or business not covered under the arrangement (unless the arrangement meets certain specified requirements).
- Records of the methodology for determining the amount of remuneration and the actual amount of remuneration paid under the arrangement must be retained for at least six years.
2. Meaningful Downside Financial Risk Exception: (Proposed 42 CFR § 411.357(aa)(2)): This exception protects remuneration paid under a value-based arrangement if the physician is at meaningful downside financial risk for failure to achieve the value-based purpose(s) of the value-based enterprise during the entire duration of the value-based arrangement. To satisfy this exception, the parties must meet the following requirements:
- The physician is responsible to pay the entity no less than 25 percent of the value of the remuneration the physician receives under the value-based arrangement or is financially responsible to the entity on a prospective basis for the cost of all or a defined set of patient care items or services.
- A description of the nature and extent of the physician’s downside risk is set forth in writing.
- The methodology used to determine the amount of remuneration is set in advance.
- The remuneration is for, or results from, value-based activities undertaken by the recipient of the remuneration for patients in the target patient population.
- The remuneration is not an inducement to reduce or limit medically necessary items or services.
- The remuneration is not conditioned on referrals of patients who are not part of the target patient population or business not covered under the arrangement (unless the arrangement meets certain specified requirements).
- Records of the methodology for determining the amount of remuneration and the actual amount of remuneration paid under the arrangement must be retained for at least six years.
3. Value-Based Arrangements Exception: (Proposed 42 CFR § 411.357(aa)(3)): This exception protects remuneration paid under a value-based arrangement if the following conditions are met:
- The arrangement is set forth in writing and signed by the parties. The writing includes a description of:
- The value-based activities to be undertaken.
- How the value-based activities are expected to further the value-based purpose of the value-based enterprise.
- The target patient population.
- The type or nature of the remuneration.
- The methodology used to determine the remuneration.
- The performance or quality standards against which the recipient will be measured.
- The performance or quality standards used are objective and measurable, and any changes to the standards must be made prospectively and in writing.
- The methodology used to determine the amount of the remuneration is set in advance.
- The remuneration is for, or results from, value-based activities undertaken by the recipient of the remuneration for patients in the target patient population.
- The remuneration is not an inducement to reduce or limit medically necessary items or services.
- The remuneration is not conditioned on referrals of patient who are not part of the target patient population or business not covered under the arrangement (unless the arrangement meets certain specified requirements).
- Records of the methodology for determining the amount of remuneration and the actual amount of remuneration paid under the arrangement must be retained for at least six years.
Soliciting Comments on Price Transparency
In the proposed rule, CMS requested comments on how to pursue its price transparency objectives in the context of the physician self-referral law. The agency notes that it is specifically interested in comments regarding the availability of pricing information and out-of-pocket costs to patients, the appropriate timing for the dissemination of pricing information and the burden associated with compliance with a requirement to provide information about factors that may affect the cost of services for which a patient is referred. CMS also seeks comments regarding whether the inclusion of a price transparency requirement in a value-based exception would provide additional patient protections against abuse.
Improving EHR and Cybersecurity Systems
CMS attempts to address several concerns surrounding arrangements between physicians and other health care providers that involve the donation of EHR and cybersecurity technology.
The agency’s proposal revises the existing EHR exception and creates a new exception for the donation of cybersecurity technology. By providing improved flexibility for these arrangements, CMS hopes to continue to foster EHR adoption and protect against cyberattacks in the health care industry.
- EHR Exception (42 CFR § 411.357(w)): This revised exception excludes nonmonetary remuneration consisting of EHR software, information technology or training services. CMS is proposing to update the rule’s requirements relating to interoperability and data lock-in; remove the sunset provision and modify certain definitions. CMS is also considering modifying or eliminating the current requirement that recipients of EHR technology contribute at least 15 percent of the technology’s costs.3
- Cybersecurity Exception (Proposed 42 CFR § 411.357(bb)): The agency is also proposing to create a new exception for the donation of cybersecurity technology and related services. CMS proposes to require that any donated cybersecurity technology and services must be documented in writing and be necessary and used predominantly to implement, maintain or reestablish cybersecurity. Such donations cannot be conditioned on or take into account the volume or value of referrals generated between the parties.4 CMS is also soliciting comments for an alternative proposal that would allow donations of cybersecurity hardware to occur if a cybersecurity risk assessment (conducted by both the recipient and the donor) has established that the hardware is reasonably necessary to protect both the donor and the recipient.5
Other Proposals
CMS also proposes a number of new rules and clarifications to existing rules meant to ease the “undue impact and burden” of the Stark Law.6 These proposals include:
- A new definition of “commercially reasonable,” (42 CFR § 411.351) which turns on whether a particular arrangement furthers a legitimate business purpose of the parties and is on similar terms and conditions as like arrangements. The revised definition does not require that an arrangement be profitable in order to be commercially reasonable.
- An objective test for determining whether compensation takes into account the volume or value of referrals or the volume or value of other business generated by the physician (42 CFR § 411.354(d)(5) and (6)). In the proposed rule, compensation would be deemed to take into account the volume or value of referrals or other business generated only if the formula used to calculate the physician’s compensation includes physicians’ referrals to the entity or other business as a variable and the physician’s compensation positively correlates with the number or value of the referrals or business.
- A revised definition of “fair market value” (42 CFR § 411.351) that eliminates the connection to the volume or value standard. CMS also proposes to modify “fair market value” to provide for a definition of general application, a definition applicable to the rental of equipment and a definition applicable to the rental of office space. As proposed, generally, “fair market value” means the value in an arm’s-length transaction with like parties and under like circumstances, of assets or services, consistent with the general market value of the subject transaction. “General market value” is defined as the price that an asset would bring as the result of bona fide bargaining by buyers and sellers who are not otherwise in a position to refer business to each other.
- A proposal to decouple Stark Law compliance from Anti-Kickback Statute compliance. The Stark Law is a strict liability statute. The Anti-Kickback Statute has an intent requirement. Many of the Stark Law’s exceptions require compliance with the Anti-Kickback Statute, which adds an “intent” element to compliance. CMS proposes to remove these requirements and expects entities to ensure compliance with both Stark and the Anti-Kickback Statute.
- A new proposed exception for limited remuneration to a physician (Proposed 42 CFR § 411.357(z)) for items or services actually provided by the physician where the remuneration does not exceed an aggregate of $3,500 provided that certain requirements are satisfied.
1 Modernizing and Clarifying the Physician Self-Referral Regulations (proposed Oct. 9, 2019) (to be published in the Federal Register), https://www.hhs.gov/sites/default/files/cms-stark-law-nprm.pdf.
2 Id. at 31.
3 Id. at 232, 234, 231.
4 Id. at 272.
5 Id. at 272–73.
6 Id. at 27.
Attachments
Authors
